Case ID: 171
Publication date: 18 Nov, 2015
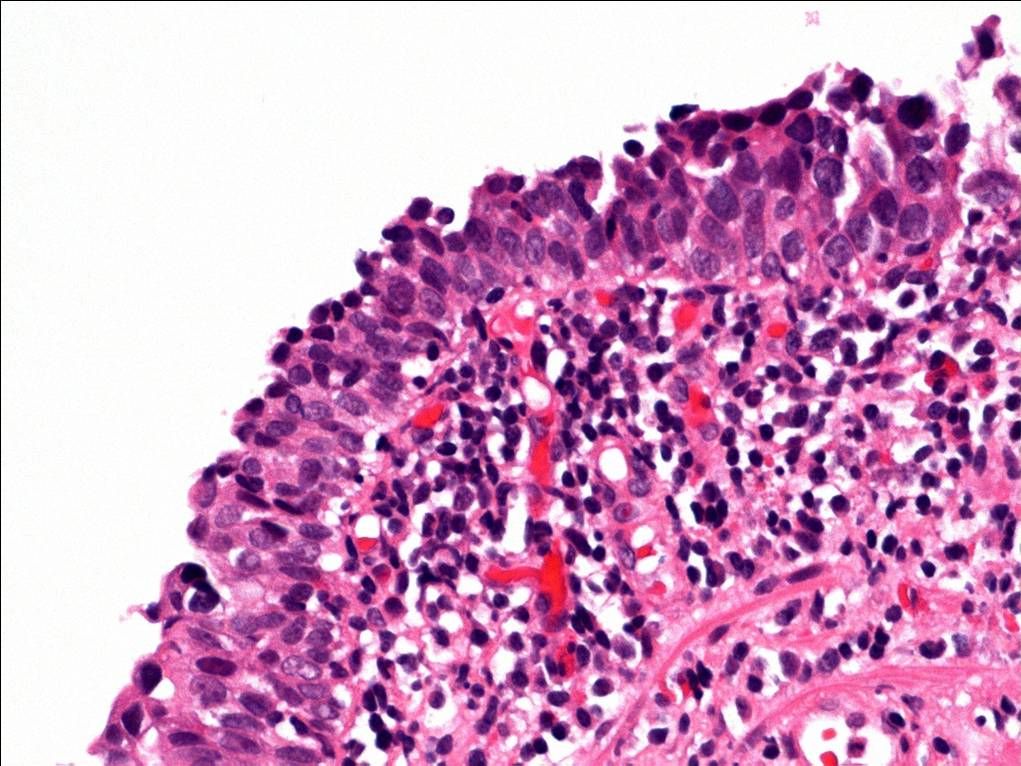
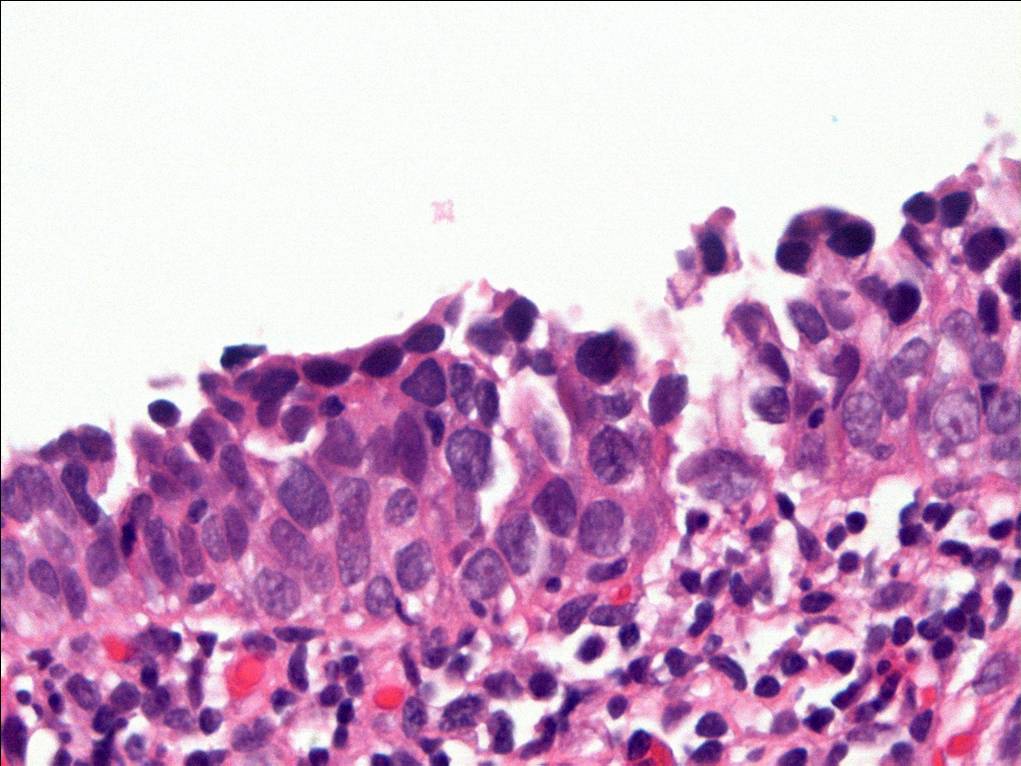
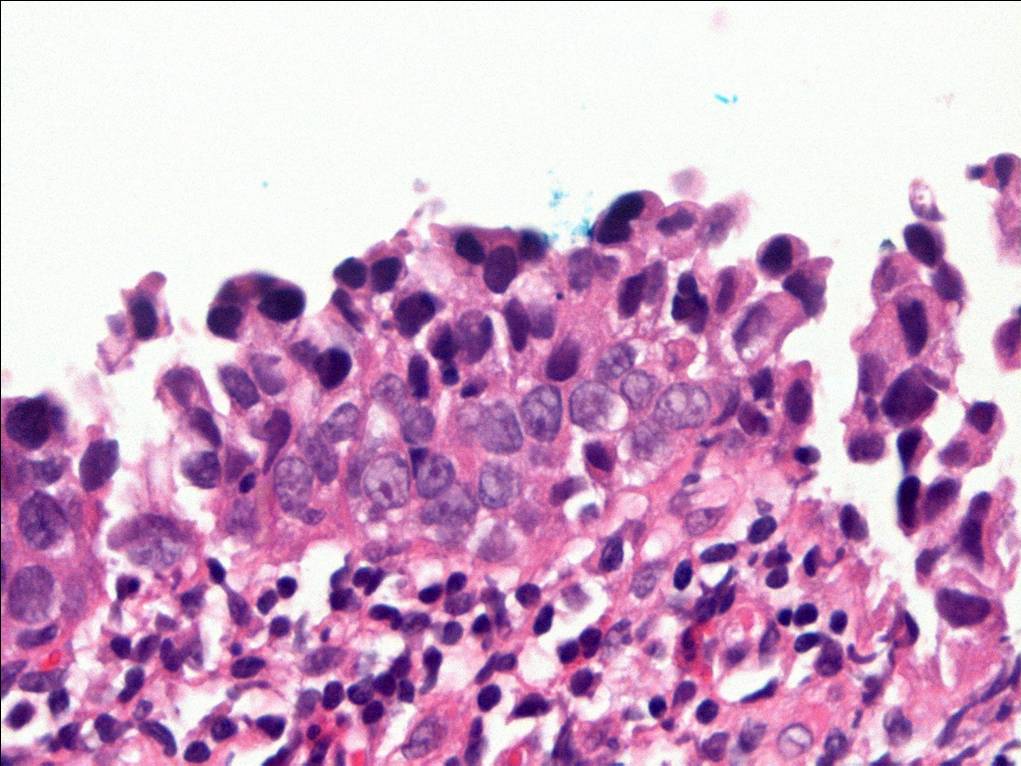
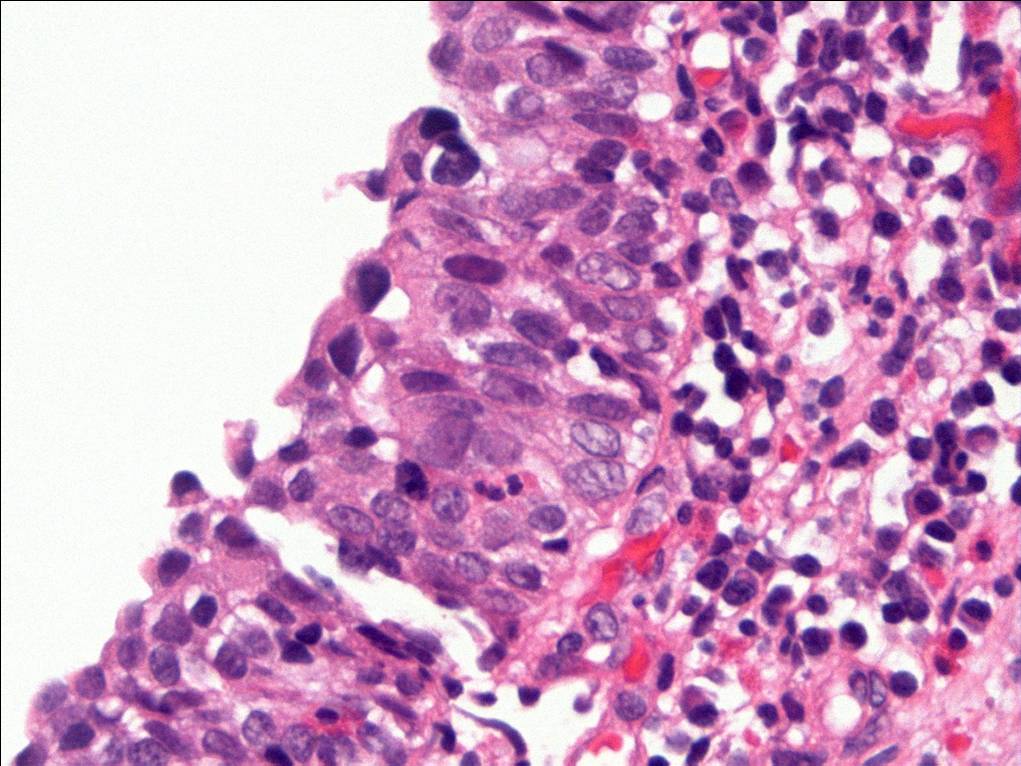
Consensus grade: Carcinoma in situ (CIS)
Show diagnosis by expert panel members| User | Diagnosis | Difficulty | Comment |
|---|---|---|---|
| Pathologist 1 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 2 | Reactive atypia | Borderline higher | |
| Pathologist 3 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 4 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 5 | Atypia/dysplasia | Borderline higher |
Quality of pics is poor |
| Pathologist 6 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 7 | Reactive atypia | Borderline higher |
Needs IHCH |
| Pathologist 8 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 9 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 10 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 11 | Atypia/dysplasia | Borderline higher | |
| Pathologist 12 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 13 | Carcinoma in situ (CIS) | Borderline lower | |
| Pathologist 14 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 15 | Reactive atypia | Typical |
No specific comment. |
| Pathologist 16 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 17 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 18 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 19 | Carcinoma in situ (CIS) | Bordering on lower | |
| Pathologist 20 | Carcinoma in situ (CIS) | Typical | |
| Pathologist 21 | Atypia/dysplasia | Bordering on higher | |
| Pathologist 22 | Carcinoma in situ (CIS) | Typical |
Some of the atypical urothelial cells present have high nuclear:cytoplasmic ratio raising the possibility of at least some element of so-called 'small cell' urohtlelial CIS (not meant to imply neuroendocrine differentiation). |
Case description (by case creator):
The degree of cytologic atypia and loss of polarity is disproportionate to the inflammation present in the lamina propria and the degree of atypia is greater than would be acceptable for reactive atypia.